Despite efforts to improve global access to basic ophthalmologic services, there remains a paucity of data regarding the prevalence of untreated ocular disease among forced migrants and refugees, particularly in east Africa. We aimed to estimate the prevalence of untreated and surgically amenable eye conditions among refugees in Nyarugusu Refugee Camp, Tanzania, and to identify factors associated with untreated eye problems. We conducted cluster-randomized sampling using the cross-sectional Surgeons OverSeas Assessment of Surgical Needs (SOSAS) survey tool to assess prevalence of surgical eye disease and access to health services among refugees in Nyarugusu from August-September 2021. Descriptive analysis and multivariable logistic regression were performed to explore associations between covariates and the presence of unresolved eye problem(s). Among 3574 refugees, 12% (n=430; mean age 36±20 yrs.) reported eye issues. Of these, 296 (69%) further characterized their problems, with 44% reporting acquired disability and 42% non-injury-related wounds. Of the 368 (86.4%) who described their issues as disabling, 78.8% endorsed a negative impact on ability to work and 27.7% required help with daily living. Most were currently (84.6%; 357/427) and chronically affected (>12 months; 88.3%; 378/428). Farming and housewife occupations were positively associated with unresolved eye problem(s). Among 312 (72.7%) who sought care, only 13 (4.2%) underwent surgery. Nearly half (136) of 279 surveyed individuals self-reported potential surgical needs, citing barriers to surgical care such as lack of available services, financial and time constraints, and limited knowledge about accessing treatment. In conclusion, nearly 1 in 8 refugees endorsed chronic and disabling eye problems, negatively impacting their work and daily life. Most who may benefit from surgery have not received care due to significant barriers and gaps in ophthalmologic services. Further investigation to better characterize specific ocular etiologies in under-resourced protracted refugee settings can inform resource allocation strategies to address unmet eye care needs.
| Published in | International Journal of Ophthalmology & Visual Science (Volume 10, Issue 1) |
| DOI | 10.11648/j.ijovs.20251001.11 |
| Page(s) | 1-15 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Refugee Health, Eye Disease, Surgical Need Asssessment, Tanzania, East Africa, Nyarugusu Refugee Camp, SOSAS Survey
Parameter | Parent Study Population | Individuals Reporting Eye Problems | ||
|---|---|---|---|---|
N | 3574 | Total: 430 | DRC: 135 | Burundi: 294 |
Average age ± SD | 23 (18) | 36 (20) | 41 (21) | 33 (19) |
Age Categories | ||||
Under 18 Years | 44 (1563 of 3544) | 19 (83 of 426) | 17 (22 of 133) | 21 (61 of 292) |
Age 18 to 29 | 26 (920 of 3544) | 26 (111 of 426) | 16 (21 of 133) | 30 (89 of 292) |
Age 30 to 44 | 17 (593 of 3544) | 22 (93 of 426) | 17 (23 of 133) | 24 (70 of 292) |
Age 45 to 59 | 8 (277 of 3544) | 16 (70 of 426) | 26 (34 of 133) | 12 (36 of 292) |
Age 60 or Older | 5 (191 of 3544) | 16 (69 of 426) | 25 (33 of 133) | 12 (36 of 292) |
Sex | ||||
Male | 43 (1547 of 3573) | 31 (132 of 430) | 39 (52 of 135) | 27 (79 of 294) |
Female | 57 (2026 of 3573) | 69 (298 of 430) | 61 (83 of 135) | 73 (215 of 294) |
Country of origin | ||||
DRC | 52 (1863 of 3568) | 31 (135 of 430) | 100 (135 of 135) | -- |
Burundi | 48 (1697 of 3568) | 68 (294 of 430) | -- | 100 (294 of 294) |
Other | 0.2 (8 of 3568) | 0 (1 of 430) | -- | -- |
Education | ||||
None | 34 (1224 of 3571) | 27 (118 of 430) | 28 (38 of 135) | 27 (80 of 294) |
Primary school | 36 (1285 of 3571) | 42 (179 of 430) | 33 (44 of 135) | 46 (135 of 294) |
Secondary school | 28 (1006 of 3571) | 30 (127 of 430) | 36 (48 of 135) | 27 (78 of 294) |
Higher education | 2 (56 of 3571) | 1 (6 of 430) | 4 (4 of 135) | <1 (1 of 294) |
Occupation | ||||
Unemployed | 63 (2256 of 3570) | 56 (242 of 429) | 57 (77 of 135) | 56 (164 of 293) |
Farmer | 13 (468 of 3570) | 19 (80 of 429) | 17 (23 of 135) | 19 (57 of 293) |
Small business | 5 (167 of 3570) | 6 (25 of 429) | 3 (4 of 135) | 7 (21 of 293) |
Domestic helper | 0.3 (11 of 3570) | 0 (1 of 429) | <1 (1 of 135) | -- |
Self-employed | 4 (153 of 3570) | 4 (17 of 429) | 3 (4 of 135) | 4 (13 of 293) |
Housewife | 5 (167 of 3570) | 7 (30 of 429) | 12 (16 of 135) | 5 (14 of 293) |
Other | 10 (348 of 3570) | 8 (34 of 429) | 7 (10 of 135) | 8 (24 of 293) |
Marital status | ||||
Married | 35 (1244 of 3561) | 50 (216 of 430) | 45 (61 of 135) | 52 (154 of 294) |
Single | 47 (1681 of 3561) | 27 (117 of 430) | 31 (42 of 135) | 26 (75 of 294) |
Divorced | 5 (167 of 3561) | 5 (22 of 430) | 6 (8 of 135) | 5 (14 of 294) |
Other | 13 (469 of 3561) | 17 (75 of 430) | 18 (24 of 135) | 17 (51 of 294) |
Religion | ||||
Christian | 93 (3326 of 3565) | 97 (416 of 430) | 94 (127 of 135) | 98 (288 of 294) |
Muslim | 5 (173 of 3565) | 2 (8 of 430) | 4 (5 of 135) | 1 (3 of 294) |
Other | 2 (66 of 3565) | 1 (6 of 430) | 2 (3 of 135) | 1 (3 of 294) |
Health indicators** | ||||
Literate | 59 (2108 of 3571) | 70 (303 of 430) | 64 (86 of 135) | 73 (216 of 294) |
Generally healthy | 79 (2802 of 3536) | 51 (219 of 427) | 56 (74 of 132) | 49 (144 of 294) |
Have ever been to a camp clinic or hospital | 92 (3297 of 3570) | 96 (414 of 430) | 97 (131 of 135) | 96 (282 of 294) |
Ill within past year | 60 (2145 of 3562) | 84 (359 of 429) | 78 (105 of 135) | 86 (253 of 293) |
Time ill in weeks* | 2 (IQR 1-4) | 4 (IQR 2-7) | 3.5 (IQR 2-8) | 4 (IQR 2-6) |
Number of visits to health center* | 2 (IQR 1-4) | 3 (IQR 2-6) | 2.5 (IQR 2-4.5) | 2 (IQR 2-6) |
Recovered from illness* | 76 (1618 of 2142) | 55 (197 of 358) | 47 (49 of 105) | 59 (148 of 252) |
Parameter | Total (N=430) |
|---|---|
Time Course (i.e., duration of symptoms) | |
0-1 months | 6 (25 of 428) |
1-12 months | 6 (25 of 428) |
>12 months (Chronic) | 88 (378 of 428) |
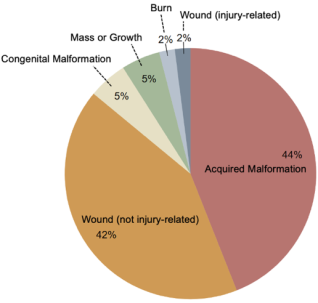
Details of Eye Problem | |
Wound (Injury or Trauma-Related) | 2 (7 of 296) |
Wound (Not Injury or Trauma-Related) | 42 (125 of 296) |
Burn | 2 (5 of 296) |
Mass or Growth | 5 (14 of 296) |
Congenital Malformation | 5 (16 of 296) |
Acquired Disability | 44 (129 of 296) |
Is the problem currently affecting you? | |
No | 16 (70 of 427) |
Yes | 84 (357 of 427) |
Is the problem debilitating? If so, in what way(s)? | |
No | 14 (58 of 426) |
Yes | 86 (368 of 426) |
I feel ashamed | 10 (38 of 368) |
I am not able to work like I used to | 79 (290 of 368) |
I need help with transportation | 15 (55 of 368) |
I need help with daily living | 28 (102 of 368) |
Did you seek healthcare for this problem? If so, what treatment(s) did you receive? | |
No | 27 (117 of 429) |
Yes | 73 (312 of 429) |
No Treatment Received | 20 (62 of 312) |
Major Procedure | 3 (8 of 312) |
Minor Procedure | 2 (5 of 312) |
Medication | 78 (242 of 312) |
Herbal Medicine | 4 (12 of 312) |
Did you see a traditional healer? | |
No | 94 (401 of 427) |
Yes | 6 (26 of 427) |
Traditional healer only | 2 (7 of 427) |
What is the primary reason you have not received eye surgery for your problem?* | |
No perceived need | 50 (138 of 274) |
No services (facilities, staff, medical equipment) | 31 (84 of 274) |
No money for treatment | 11 (31 of 274) |
Did not know about access to treatment | 4 (11 of 274) |
No time to receive treatment | 2 (5 of 274) |
Fear/mistrust | 1 (3 of 274) |
No money for travel | <1 (2 of 274) |
Covariates | OR | 95% CI | P-value |
|---|---|---|---|
Age Category | |||
Under 18 | REF | - | - |
18 to 29 | 0.39 | 0.13 - 1.16 | 0.089 |
30 to 44 | 0.50 | 0.15 - 1.73 | 0.275 |
45 to 59 | 0.94 | 0.24 - 3.66 | 0.932 |
60 or Older | 1.94 | 0.44 - 8.58 | 0.380 |
Sex | |||
Male | REF | - | - |
Female | 0.88 | 0.45 - 1.74 | 0.716 |
Country of origin | |||
Burundi | REF | - | - |
DRC | 0.69 | 0.33 - 1.43 | 0.317 |
Education | |||
None | 0.22 | 0.04 - 1.30 | 0.094 |
Primary school | 0.72 | 0.34 - 1.51 | 0.378 |
Secondary school | REF | - | - |
Higher education (college diploma) | 0.38 | 0.03 - 5.28 | 0.468 |
Occupation | |||
Unemployed | REF | - | - |
Farmer | 2.88* | 1.17 - 7.09 | 0.022 |
Small Business Owner | 1.78 | 0.54 - 5.91 | 0.347 |
Self-Employed | 0.45 | 0.13 - 1.50 | 0.192 |
Domestic Helper a | - | - | - |
Housewife (mother of the home) | 5.26* | 1.08 - 25.53 | 0.039 |
Other | 2.08 | 0.65 - 6.68 | 0.219 |
Marital status | |||
Married | REF | - | - |
Single | 1.23 | 0.47 - 3.26 | 0.671 |
Divorced | 5.97 | 0.68 - 52.20 | 0.106 |
Other | 0.93 | 0.38 - 2.28 | 0.872 |
Religion | |||
Christian | REF | - | - |
Muslim | 0.61 | 0.06 - 6.07 | 0.675 |
Other b | - | - | - |
Literate | |||
No | REF | - | - |
Yes | 0.22 | 0.04 - 1.17 | 0.077 |
Generally Healthy? | |||
No | REF | - | - |
Yes | 1.51 | 0.80 - 2.84 | 0.206 |
Use PHC? | |||
No | REF | - | - |
Yes | 0.11 | 0.01 - 1.04 | 0.054 |
Illness Past Year | |||
No | REF | - | - |
Yes | 1.91 | 0.84 - 4.33 | 0.121 |
Timing of Eye Problem | |||
Last Month | 0.89 | 0.25 - 3.20 | 0.857 |
Between 1-12 Months Back | 0.41 | 0.13 - 1.24 | 0.113 |
Over 12 Months Back | REF | - | - |
VI | Vision Impairment |
SOSAS | Surgeons OverSeas Assessment of Surgical Needs |
LMIC | Low- and Middle-Income Countries |
OR | Odds Ratio |
CI | Confidence Interval |
NGO | Nongovernmental Organization |
CHW | Community Health Worker |
AMO-O | Assistant Medical Officer Ophthalmologist |
HSSP | Health Sector Strategic Plan |
TZS | Tanzanian Shilling |
USD | United States Dollar |
NSOAP | National Surgical, Obstetric, and Anesthesia Plan |
SOA | Surgical, Obstetric, and Anesthesia |
| [1] | Burton MJ, Ramke J, Marques AP, et al. The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. Lancet Glob Health. 2021; 9(4): e489-e551. |
| [2] | GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021; 9(2): e130-e143. |
| [3] |
Vision impairment and blindness. Accessed January 21, 2024.
https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment |
| [4] | Marques AP, Ramke J, Cairns J, et al. Global economic productivity losses from vision impairment and blindness. EClinicalMedicine. 2021; 35: 100852. |
| [5] |
Eye Care Foundation’s NURU Project. The International Agency for the Prevention of Blindness. Accessed September 12, 2024.
https://www.iapb.org/blog/eye-care-foundations-nuru-project/ |
| [6] | Ahmed M, Whitestone N, Patnaik JL, et al. Burden of eye disease and demand for care in the Bangladesh Rohingya displaced population and host community: A cohort study. PLoS Med. 2020; 17(3): e1003096. |
| [7] | Gelaw Y, Abateneh A. Ocular morbidity among refugees in Southwest Ethiopia. Ethiop J Health Sci. 2014; 24(3): 227-234. |
| [8] | Kawuma M. Eye diseases and blindness in Adjumani refugee settlement camps, Uganda. East Afr Med J. 2000; 77(11): 580-582. |
| [9] | Awan H, T I. Prevalence of visual impairment and eye diseases in Afghan refugees in Pakistan. Eastern Mediterranean Health Journal. 1998; 4: 560-566. |
| [10] | Kaphle D, Gyawali R, Kandel H, Reading A, Msosa JM. Vision Impairment and Ocular Morbidity in a Refugee Population in Malawi. Optometry and Vision Science. 2016; 93(2): 188. |
| [11] | Hashemi H, Yekta A, Jafarzadehpur E, Doostdar A, Ostadimoghaddam H, Khabazkhoob M. The prevalence of visual impairment and blindness in underserved rural areas: a crucial issue for future. Eye (Lond). 2017; 31(8): 1221-1228. |
| [12] | Refugee Data Finder. UNHCR. Accessed January 21, 2024. |
| [13] | Bal S, Duckles A, Buttenheim A. Visual Health and Visual Healthcare Access in Refugees and Displaced Persons: A Systematic Review. Journal of Immigrant and Minority Health. 2019; 21(1): 161-174. |
| [14] |
Protracted Refugee Situations Explained. Accessed March 20, 2024.
https://www.unrefugees.org/news/protracted-refugee-situations-explained/ |
| [15] | Tanzania Refugee Population Update (as of 30 June 2024) - United Republic of Tanzania | ReliefWeb. July 15, 2024. Accessed August 1, 2024. |
| [16] | Enumah ZO, Manyama F, Yenokyan G, et al. Untreated Surgical Problems Among East African Refugees: A Cluster Randomized, Cross-Sectional Study. World J Surg. 2022; 46(6): 1278-1287. |
| [17] | Moustafa MK, Al-Hajj S, El-Hechi M, El Moheb M, Chamseddine Z, Kaafarani HMA. The Burden of Surgical Disease and Access to Care in a Vulnerable Syrian Refugee Population in Lebanon. World Journal of Surgery. 2021; 45(10): 1. |
| [18] | Resources. Surgeons Overseas. Accessed August 8, 2024. |
| [19] | Rapoza PA, West SK, Katala SJ, Taylor HR. Prevalence and causes of vision loss in central Tanzania. Int Ophthalmol. 1991; 15(2): 123-129. |
| [20] | Jolley E, Buttan S, Engels T, et al. Prevalence of Visual Impairment and Coverage of Cataract Surgical Services: Associations with Sex, Disability, and Economic Status in Five Diverse Sites. Ophthalmic Epidemiology. 2020; 27(6): 429-437. |
| [21] | Bin Yameen TA, Abadeh A, Lichter M. Visual impairment and unmet eye care needs among a Syrian pediatric refugee population in a Canadian city. Canadian Journal of Ophthalmology. 2019; 54(6): 668-673. |
| [22] | Bin Yameen TA, Abadeh A, Slomovic J, Lichter M. Visual impairment and unmet eye care needs among a Syrian adult refugee population in a Canadian city. Canadian Journal of Ophthalmology. 2020; 55(2): 137-142. |
| [23] | Erdem S. Causes of Blindness among Syrian Refugees Living in Southeastern Turkey. Ophthalmic Epidemiology. 2019; 26(6): 416-419. |
| [24] | Abou-Gareeb I, Lewallen S, Bassett K, Courtright P. Gender and blindness: a meta-analysis of population-based prevalence surveys. Ophthalmic Epidemiol. 2001; 8(1): 39-56. |
| [25] | Naidoo K, Gichuhi S, Basáñez MG, et al. Prevalence and causes of vision loss in sub-Saharan Africa: 1990-2010. British Journal of Ophthalmology. 2014; 98(5): 612-618. |
| [26] | Courtright P, West SK. Contribution of sex-linked biology and gender roles to disparities with trachoma. Emerg Infect Dis. 2004; 10(11): 2012-2016. |
| [27] | Seddon J, Fong D, West SK, Valmadrid CT. Epidemiology of risk factors for age-related cataract. Survey of Ophthalmology. 1995; 39(4): 323-334. |
| [28] | Alene GD, Abebe S. Prevalence of risk factors for trachoma in a rural locality of north-western Ethiopia. East Afr Med J. 2000; 77(6): 308-312. |
| [29] | Szewczyk M, Pazdrowski J, Golusiński P, et al. Basal cell carcinoma in farmers: an occupation group at high risk. Int Arch Occup Environ Health. 2016; 89(3): 497-501. |
| [30] | Jesudason T. Reducing trachoma in women. The Lancet Infectious Diseases. 2023; 23(6): 660. |
| [31] | Sanders A, Emerson P, Courtright P, Hooper P. Women and trachoma: why prioritising gender equity is essential to achieve vision for all. Community Eye Health. 2023; 36(119): 19. |
| [32] | Congdon N, West S, Vitale S, Katala S, Mmbaga BB. Exposure to children and risk of active trachoma in Tanzanian women. Am J Epidemiol. 1993; 137(3): 366-372. |
| [33] | Murdoch I, Smith AF, Baker H, Shilio B, Dhalla K. The cost and quality of life impact of glaucoma in Tanzania: An observational study. PLoS One. 2020; 15(6): e0232796. |
| [34] | Guchi GS, Mersha GA, Alimaw YA, Assem AS, Fekadu SA. Vision-Related Quality of Life and Associated Factors Among an Adult Population with Glaucoma Attending a Comprehensive Specialized Hospital, Northwest Ethiopia. Clin Ophthalmol. 2023; 17: 225-237. |
| [35] | Otache AE, Ezenwosu IL, Ossai EN, Aniwada EC, Nwobi EA, Uzochukwu BSC. Health-related quality of life and associated factors among Onchocerciasis patients in southeast Nigeria: A cross-sectional comparative study. PLoS Negl Trop Dis. 2022; 16(2): e0010182. |
| [36] | Assi L, Chamseddine F, Ibrahim P, et al. A Global Assessment of Eye Health and Quality of Life: A Systematic Review of Systematic Reviews. JAMA Ophthalmol. 2021; 139(5): 526-541. |
| [37] | Abrahim O, Rapaport S, Ngude H, et al. Patterns of referral for refugees in western Tanzania: a retrospective review. Pan Afr Med J. 2022; 41: 76. |
| [38] | Weerasuriya CK, Tan SO, Alexakis LC, et al. Evaluation of a surgical service in the chronic phase of a refugee camp: an example from the Thai-Myanmar border. Conflict and Health. 2012; 6(1): 95. |
| [39] | Hussain AHME, Ahmed M, Vincent JE, et al. Rapid assessment of avoidable blindness and cataract surgery coverage among forcibly displaced Myanmar Nationals (Rohingya refugees) in Cox’s Bazar, Bangladesh. PLoS One. 2020; 15(12): e0243005. |
| [40] | Zeidan Z, Hashim K, Muhit MA, Gilbert C. Prevalence and causes of childhood blindness in camps for displaced persons in Khartoum: results of a household survey. East Mediterr Health J. 2007; 13(3): 580-585. |
| [41] | Whoever, Wherever, Whenever: Improving Access to Quality Eye Care for Forcibly Displaced Populations. The International Agency for the Prevention of Blindness. Accessed August 29, 2024. |
| [42] | Anderson JDC, Bentley CC. Role of Community Health Workers in Trachoma Control: Case Study from a Somali Refugee Camp. Trop Doct. 1986; 16(2): 66-69. |
| [43] | Dean WH, Buchan JC, Gichuhi S, et al. Ophthalmology training in sub-Saharan Africa: a scoping review. Eye (Lond). 2021; 35(4): 1066-1083. |
| [44] | Goodell AJ, Kahn JG, Ndeki SS, Kaale E, Kaaya EE, Macfarlane SBJ. Modeling solutions to Tanzania’s physician workforce challenge. Glob Health Action. 2016; 9. |
| [45] | Old_National Surgical Planning. pgssc. Accessed March 6, 2024. |
| [46] | Ramke J, Evans JR, Habtamu E, et al. Grand Challenges in global eye health: a global prioritisation process using Delphi method. Lancet Healthy Longev. 2022; 3(1): e31-e41. |
| [47] | Taylor HR, Burton MJ, Haddad D, West S, Wright H. Trachoma. The Lancet. 2014; 384(9960): 2142-2152. |
| [48] | Foster A, Yorston D. Corneal ulceration in Tanzanian children: Relationship between measles and vitamin A deficiency. Transactions of The Royal Society of Tropical Medicine and Hygiene. 1992; 86(4): 454-455. |
| [49] | Grant GB, Desai S, Dumolard L, Kretsinger K, Reef SE. Progress Toward Rubella and Congenital Rubella Syndrome Control and Elimination — Worldwide, 2000-2018. MMWR Morb Mortal Wkly Rep. 2019; 68(39): 855-859. |
| [50] | Solomon AW, Akudibillah J, Abugri P, et al. Pilot study of the use of community volunteers to distribute azithromycin for trachoma control in Ghana. Bull World Health Organ. 2001; 79(1): 8-14. |
| [51] | Tekle AH, Zouré HGM, Noma M, et al. Progress towards onchocerciasis elimination in the participating countries of the African Programme for Onchocerciasis Control: epidemiological evaluation results. Infect Dis Poverty. 2016; 5: 66. |
| [52] | Frick KD, Riva-Clement L, Shankar MB. Screening for refractive error and fitting with spectacles in rural and urban India: cost-effectiveness. Ophthalmic Epidemiol. 2009; 16(6): 378-387. |
| [53] | Reddy PA, Congdon N, MacKenzie G, et al. Effect of providing near glasses on productivity among rural Indian tea workers with presbyopia (PROSPER): a randomised trial. Lancet Glob Health. 2018; 6(9): e1019-e1027. |
| [54] | Glewwe P, Park A, Zhao M. A better vision for development: Eyeglasses and academic performance in rural primary schools in China. Journal of Development Economics. 2016; 122: 170-182. |
| [55] | Ma X, Zhou Z, Yi H, et al. Effect of providing free glasses on children’s educational outcomes in China: cluster randomized controlled trial. BMJ. 2014; 349: g5740. |
| [56] | Sabherwal S, Sood I, Siddiqui Z, DasGupta S, Ganesh S, Basset K. Out-of-School Vision Screening in North India: Estimating the Magnitude of Need. Ophthalmic Epidemiology. 2020; 27(6): 449-452. |
| [57] | Vincent JE, Netek S, Parry A, Mladenovich D, Thein NN, Amendola PR. Reported Wearing Compliance of Ready-Made Spectacles at 6 and 12 Months. Optometry and Vision Science. 2010; 87(12): 958. |
| [58] | Vincent JE. Simple Spectacles for Adult Refugees on the Thailand-Burma Border. Optometry and Vision Science. 2006; 83(11): 803. |
| [59] | Morjaria P, McCormick I, Gilbert C. Compliance and Predictors of Spectacle Wear in Schoolchildren and Reasons for Non-Wear: A Review of the Literature. Ophthalmic Epidemiol. 2019; 26(6): 367-377. |
| [60] | Mavrakanas N, Dhalla KA, Jecha J, Kapesa I, Odouard C, Murdoch I. Results and safety profile of trainee cataract surgeons in a community setting in East Africa. Indian J Ophthalmol. 2016; 64(11): 818-821. |
| [61] | WHO Model Lists of Essential Medicines. Accessed August 29, 2024. |
| [62] | Newman-Casey PA, Niziol LM, Gillespie BW, Janz NK, Lichter PR, Musch DC. The Association between Medication Adherence and Visual Field Progression in the Collaborative Initial Glaucoma Treatment Study (CIGTS). Ophthalmology. 2020; 127(4): 477-483. |
| [63] | Che Hamzah J, Daka Q, Azuara-Blanco A. Home monitoring for glaucoma. Eye (Lond). 2020; 34(1): 155-160. |
| [64] | Courtright P, Murenzi J, Mathenge W, Munana J, Müller A. Reaching rural Africans with eye care services: findings from primary eye care approaches in Rubavu District, Rwanda. Tropical Medicine & International Health. 2010; 15(6): 692-696. |
| [65] | Rono H, Bastawrous A, Macleod D, et al. Smartphone-Guided Algorithms for Use by Community Volunteers to Screen and Refer People With Eye Problems in Trans Nzoia County, Kenya: Development and Validation Study. JMIR mHealth and uHealth. 2020; 8(6): e16345. |
| [66] | Upadhyay M, Karmacharya P, Koirala S, et al. The Bhaktapur eye study: ocular trauma and antibiotic prophylaxis for the prevention of corneal ulceration in Nepal. Br J Ophthalmol. 2001; 85(4): 388-392. |
| [67] | United Republic of Tanzania. UNHCR. Accessed March 7, 2024. |
| [68] | admin. Health Sector Strategic Plan July 2021 - June 2026 (HSSP V). MITU. July 12, 2021. Accessed March 6, 2024. |
| [69] | Malik ANJ, Mafwiri M, Gilbert C. Integrating primary eye care into global child health policies. Arch Dis Child. 2018; 103(2): 176-180. |
| [70] |
Costing of Tanzania’s Health Sector Strategic Plan V 2020/21-2025/26: Estimated Cost and Impact of the Plan. Accessed August 24, 2024.
http://www.healthpolicyplus.com/ns/pubs/18550-18972_HSSPVCosting.pdf |
| [71] |
Sustainability Implications for Tanzania’s Fourth Health Sector Strategic Plan, 2015/16-2019/20. Accessed August 24, 2024.
https://www.healthpolicyproject.com/pubs/527_FINALTZOneHealthreport.pdf |
| [72] | Citron I, Jumbam D, Dahm J, et al. Towards equitable surgical systems: development and outcomes of a national surgical, obstetric and anaesthesia plan in Tanzania. BMJ Global Health. 2019; 4(2): e001282. |
| [73] | Hellar AM, Akoko L, Jumbam DT, et al. An Assessment of Progress and Challenges in the Implementation of the National Surgical, Obstetric, and Anesthesia Plan (NSOAP) in Tanzania. East Cent Afr J Surg. 2024; 29(2): 15-22. |
APA Style
Wang, D., Reddy, A., Anant, S., Rafiq, M. Y., Juma, O., et al. (2025). Prevalence and Characteristics of Eye Problems Reported in an East African Refugee Camp: A Cross-Sectional Survey. International Journal of Ophthalmology & Visual Science, 10(1), 1-15. https://doi.org/10.11648/j.ijovs.20251001.11
ACS Style
Wang, D.; Reddy, A.; Anant, S.; Rafiq, M. Y.; Juma, O., et al. Prevalence and Characteristics of Eye Problems Reported in an East African Refugee Camp: A Cross-Sectional Survey. Int. J. Ophthalmol. Vis. Sci. 2025, 10(1), 1-15. doi: 10.11648/j.ijovs.20251001.11
@article{10.11648/j.ijovs.20251001.11,
author = {Dorothy Wang and Ashwin Reddy and Shruti Anant and Mohamed Yunus Rafiq and Omar Juma and Hilary Ngude and Frank Manyama and Alexander Blum and Joseph Sakran and Kent Stevens and Ruth Tessema and Zachary Obinna Enumah},
title = {Prevalence and Characteristics of Eye Problems Reported in an East African Refugee Camp: A Cross-Sectional Survey
},
journal = {International Journal of Ophthalmology & Visual Science},
volume = {10},
number = {1},
pages = {1-15},
doi = {10.11648/j.ijovs.20251001.11},
url = {https://doi.org/10.11648/j.ijovs.20251001.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijovs.20251001.11},
abstract = {Despite efforts to improve global access to basic ophthalmologic services, there remains a paucity of data regarding the prevalence of untreated ocular disease among forced migrants and refugees, particularly in east Africa. We aimed to estimate the prevalence of untreated and surgically amenable eye conditions among refugees in Nyarugusu Refugee Camp, Tanzania, and to identify factors associated with untreated eye problems. We conducted cluster-randomized sampling using the cross-sectional Surgeons OverSeas Assessment of Surgical Needs (SOSAS) survey tool to assess prevalence of surgical eye disease and access to health services among refugees in Nyarugusu from August-September 2021. Descriptive analysis and multivariable logistic regression were performed to explore associations between covariates and the presence of unresolved eye problem(s). Among 3574 refugees, 12% (n=430; mean age 36±20 yrs.) reported eye issues. Of these, 296 (69%) further characterized their problems, with 44% reporting acquired disability and 42% non-injury-related wounds. Of the 368 (86.4%) who described their issues as disabling, 78.8% endorsed a negative impact on ability to work and 27.7% required help with daily living. Most were currently (84.6%; 357/427) and chronically affected (>12 months; 88.3%; 378/428). Farming and housewife occupations were positively associated with unresolved eye problem(s). Among 312 (72.7%) who sought care, only 13 (4.2%) underwent surgery. Nearly half (136) of 279 surveyed individuals self-reported potential surgical needs, citing barriers to surgical care such as lack of available services, financial and time constraints, and limited knowledge about accessing treatment. In conclusion, nearly 1 in 8 refugees endorsed chronic and disabling eye problems, negatively impacting their work and daily life. Most who may benefit from surgery have not received care due to significant barriers and gaps in ophthalmologic services. Further investigation to better characterize specific ocular etiologies in under-resourced protracted refugee settings can inform resource allocation strategies to address unmet eye care needs.
},
year = {2025}
}
TY - JOUR T1 - Prevalence and Characteristics of Eye Problems Reported in an East African Refugee Camp: A Cross-Sectional Survey AU - Dorothy Wang AU - Ashwin Reddy AU - Shruti Anant AU - Mohamed Yunus Rafiq AU - Omar Juma AU - Hilary Ngude AU - Frank Manyama AU - Alexander Blum AU - Joseph Sakran AU - Kent Stevens AU - Ruth Tessema AU - Zachary Obinna Enumah Y1 - 2025/03/06 PY - 2025 N1 - https://doi.org/10.11648/j.ijovs.20251001.11 DO - 10.11648/j.ijovs.20251001.11 T2 - International Journal of Ophthalmology & Visual Science JF - International Journal of Ophthalmology & Visual Science JO - International Journal of Ophthalmology & Visual Science SP - 1 EP - 15 PB - Science Publishing Group SN - 2637-3858 UR - https://doi.org/10.11648/j.ijovs.20251001.11 AB - Despite efforts to improve global access to basic ophthalmologic services, there remains a paucity of data regarding the prevalence of untreated ocular disease among forced migrants and refugees, particularly in east Africa. We aimed to estimate the prevalence of untreated and surgically amenable eye conditions among refugees in Nyarugusu Refugee Camp, Tanzania, and to identify factors associated with untreated eye problems. We conducted cluster-randomized sampling using the cross-sectional Surgeons OverSeas Assessment of Surgical Needs (SOSAS) survey tool to assess prevalence of surgical eye disease and access to health services among refugees in Nyarugusu from August-September 2021. Descriptive analysis and multivariable logistic regression were performed to explore associations between covariates and the presence of unresolved eye problem(s). Among 3574 refugees, 12% (n=430; mean age 36±20 yrs.) reported eye issues. Of these, 296 (69%) further characterized their problems, with 44% reporting acquired disability and 42% non-injury-related wounds. Of the 368 (86.4%) who described their issues as disabling, 78.8% endorsed a negative impact on ability to work and 27.7% required help with daily living. Most were currently (84.6%; 357/427) and chronically affected (>12 months; 88.3%; 378/428). Farming and housewife occupations were positively associated with unresolved eye problem(s). Among 312 (72.7%) who sought care, only 13 (4.2%) underwent surgery. Nearly half (136) of 279 surveyed individuals self-reported potential surgical needs, citing barriers to surgical care such as lack of available services, financial and time constraints, and limited knowledge about accessing treatment. In conclusion, nearly 1 in 8 refugees endorsed chronic and disabling eye problems, negatively impacting their work and daily life. Most who may benefit from surgery have not received care due to significant barriers and gaps in ophthalmologic services. Further investigation to better characterize specific ocular etiologies in under-resourced protracted refugee settings can inform resource allocation strategies to address unmet eye care needs. VL - 10 IS - 1 ER -
Center for Global Surgery, Department of Surgery, Johns Hopkins University, Baltimore, The United States
Center for Global Surgery, Department of Surgery, Johns Hopkins University, Baltimore, The United States
Center for Global Surgery, Department of Surgery, Johns Hopkins University, Baltimore, The United States
Department of Anthropology, New York University, Shanghai, China
Ifakara Health Institute, Bagamoyo, Tanzania
Tanzania Red Cross Society, Dar es Salaam, Tanzania
Tanzania Red Cross Society, Dar es Salaam, Tanzania
Center for Global Surgery, Department of Surgery, Johns Hopkins University, Baltimore, The United States
Center for Global Surgery, Department of Surgery, Johns Hopkins University, Baltimore, The United States
Center for Global Surgery, Department of Surgery, Johns Hopkins University, Baltimore, The United States
Department of Ophthalmology, Johns Hopkins University, Baltimore, The United States
Center for Global Surgery, Department of Surgery, Johns Hopkins University, Baltimore, The United States; Department of International Health, Johns Hopkins University, Baltimore, The United States